5-10% of the smallest premature infants develop necrotizing enterocolitis (NEC), a potentially lethal disorder in which portions of the bowel undergo tissue death. A key goal in the treatment of preterm infants is achievement of full enteral feeding as early as possible to optimize growth (and to improve longer term clinical outcomes.
Necrotizing enterocolitis and feeding tolerance
Necrotizing enterocolitis (NEC) is a serious inflammatory disease of the gastrointestinal system of the premature infant in which portions of the bowel undergo tissue death (necrosis). It has an unpredictable, acute onset and today operative resection of the affected intestinal segments is the only specific treatment.
NEC is a leading cause of morbidity and mortality among premature infants in neonatal intensive care units. Approximately 3,700 and 1,500 infants in Europe and in the US, respectively die every year from the complications of NEC.
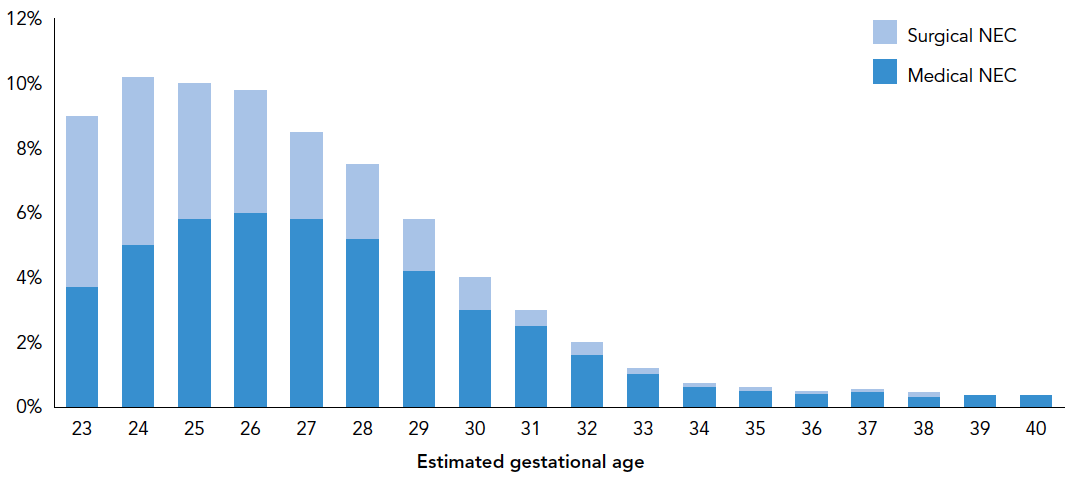
NEC almost exclusively affects premature infants and the most significant risk factor for its development is the degree of prematurity of the infant; the lower the birth weight and gestational age at birth are, the higher risk for NEC becomes.
The figure below shows the proportion of newborn babies in different age groups (estimated week of gestational age) developing NEC requiring supportive medical treatment only (Medical NEC) and those where abdominal operation (Surgical NEC) becomes necessary (from Clark et al. 2012).
Not only is the risk of developing NEC higher for the smallest premature infants, but the risk of dying from NEC also is the highest for the smallest and most premature babies.
The figure below shows the proportion of babies that died from NEC in relation to their estimated gestational age at birth. Numbers in parentheses describe the total number of investigated babies within each gestational age group (from Clark et al. 2012).

The longer-term consequences for premature infants developing NEC vary from none to short bowel syndrome, abnormal growth, and impaired neurodevelopment including cerebral palsy, cognitive impairment, visual impairment, and hearing impairment.
Treatment and Prevention of NEC
Despite decades of research, there is still no definitive therapy available today to prevent NEC from happening. There is no well-recognized cause for the development of NEC besides the risk factors of immaturity of the premature bowel with respect to e.g. innervation, immunologic capability, motility and bacterial colonization. Current medical interventions are supportive and aimed at limiting ventilatory, circulatory, infectious and other complications of the bowel necrosis. Such strategies currently include e.g. early entry of oral feeding, especially with human milk, abdominal massage and attempts to limit the use of antibiotics, none of which has a consistently proven effect.
Thus, prophylaxis for NEC represents a true unmet medical need. Given that NEC predominantly affects the most vulnerable premature infants, the development of preventive NEC strategies are highly prioritized.
The neonatal intensive care environment favours the growth of pathogenic, potentially dangerous bacteria in the developing gastrointestinal tract, which may elevate the risk of contracting not only NEC, but also potentially lethal infections. Blooms of such pathogenic bacteria have been seen in the gut of preterm infants in the days before they get NEC. This has led to the hypothesis and clinical testing of the concept of providing live, beneficial (i.e. probiotic) bacteria into the preterm infant gut early in life might prevent growth of such harmful bacteria and thereby limit the risk of developing NEC.
Despite years of research, there is still currently no medical drug formulation of live bacteria that has undergone medical agency approved, rigorous pharmaceutical production and clinical risk and benefit-testing, all of which are mandatory for any substance or agent that is to be used to cure, mitigate, treat or prevent disease. IBT is alone in such a development with its drug candidate IBP-9414 for the prevention of NEC.
Feeding Tolerance
The first weeks of nutrition have important implications for the development of prematurely born infants. The goal of achieving early and adequate enteral nutrition in these infants is to facilitate recovery or catch up growth, to achieve normal body composition, whilst minimizing undesirable effects of nutritional imbalances (e.g. hyperglycemia, insulin resistance, etc.). Improved feeding tolerance and achievement of full enteral feeding as early as possible is expected to optimize growth. Evidence-based guidelines for nutrition of the VLBW infant (Murgas-Torrazza, 2013), recommend starting parenteral nutrition within the first hours postnatally as the immature gastrointestinal tract is not ready to accept full enteral feedings in these infants directly after birth. However, prolonged parenteral (intravenous) nutrition (particularly with lipids) is associated with complications (intrahepatic cholestasis, increased risk of bronchopulmonary dysplasia, worsening of pulmonary vascular resistance, intravenous line-mediated infections and sepsis.
The enteral route is the most physiological and natural way of administering nutrients to the neonate. The introduction of enteral feeding is therefore recommended as soon as possible, and ideally on day 1 with the goal of reaching full volume feedings at 120 ml/kg/day to support growth as quickly as clinically feasible. This not only minimizes the need for parenteral nutrition and the associated risks of complications, but also the administration of enteral feed in the developing gut has long been known to combat intestinal atrophy. Establishing sustained enteral feeding, associated with the discontinuation of parenteral nutrition is thus one of the most important goals, especially in VLBW and ELBW infants. Reducing the time to reach this goal, even with only 1 or 2 days less, is considered to be clinically important in the development of the preterm infant.
During the first 14 days of life, measured body weight can be very variable in premature infants and can be influenced by oedema and multiple morbidities. However, after the first 2 weeks, true weight gain is reflected by body weight. Steady growth is expected from the time full enteral feeding is established and until the infant can leave the hospital. Thus, achieving sustained feeding tolerance with full enteral feeding, together with the associated benefit of the permanent discontinuation of parenteral nutrition and steady growth when treated with IBP-9414 would be a major beneficial contribution to a favourable clinical outcome in preterm infants.